Introduction
Guidelines for resuscitation have been published widely for more than 30 years and since the advent of evidence-based medicine, the development of such guidelines has been achieved through consensus amongst renowned global experts organised by the International Liaison Committee on Resuscitation (ILCOR). Since 2000, comprehensive resuscitation guidelines have been published every 5 years, most recently in October 2015.
A rigorous evidence-based approach was applied to this guideline development, which used the GRADE system (Guyatt, et al, 2008) alongside the ‘population / patient / problem – intervention – comparator – outcome (PICO) method (Center for Evidence Based Medicine, 2009) of identifying published, peer reviewed evidence in order to achieve a consensus on science – the evidence was divided amongst a number of subject specific task forces constructed from a wide range of learned, experienced and committed professionals (Nolan, et al, 2015).
Contemporary clinical guidelines are purposefully constructed to be deliverable and fit for purpose. A key element is the implementation and integration of those guidelines into clinical practice. Accordingly it is necessary to place strong emphasis on getting the message across, transferring the evidence into practice and (hopefully) improving patient outcomes. In the field of resuscitation this is largely achieved through the educational medium of (didactic) life support courses. The education delivered during life support courses is conducted by a cadre of instructors who are required to have successfully completed an instructor course and be subject to peer review / re-certification in 4 yearly cycles.
Whilst it is evident that in addition to the considerable investment and input into education & training, improvements in technology have also influenced guideline development, however, patient outcomes and survivorship from in-hospital cardiac arrest have remained largely unchanged at around 18% (Gwinnutt et al, 2000, Peberdy et al, 2003, Nolan, 2014).
Non-Technical Skills / Human Factors
It is well known that critical care environments, where quick decisions have to be made under intense pressure are a common source of avoidable error and patient-harm (Bucknall, 2010). A recent study by Patterson and colleagues (2015) identified a series of behavioural components that are culturally embedded within the practice of emergency care, which remain poorly understood.
The authors identified the following key characteristics of emergency care that influence (perhaps untrained) human behaviour in ‘high-pressure’ situations;
- Conditions change quickly
- Disruptions and distractions are common
- Poor communication and / or under-developed teamwork are common
- Hospital teams are pseudo-teams as team membership is inconsistent and changes frequently, with little or no pre-established professional rapport.
- Different professional cultures exist
- Different perceptions
- Different perspectives
- Intra-professional tensions
- Crisis management
- Under-developed organisational skills
- Lack of experience & situational awareness
- Incomplete procedural standardisation (e.g. ABCDE assessment, SBAR)
The features highlighted above are recognisable and perhaps typical in medical emergency events and certainly not limited to the emergency department.
Nature and source of error in sub-optimal performance of skills
There are very many publications that outline significant human factors related failures that emerge during attempts to deliver optimal treatment, many indicate guideline deviations, and Reason (1990) described these as attributable to slips, lapses, mistakes and violations.
Recent technological advancements that have enabled defibrillators to capture objective, real-time, in-the-field data has been very useful in that it has provided unique insights into the behaviours of resuscitation teams and actual resuscitation practice.
Publications that have examined detailed data from defibrillator downloads have identified an array of real-time performance errors. Examples of such errors have included inadequate chest compression depth, slow compression rates and incomplete release of the chest (Whitfield et al, 2005, Abella et al, 2007). Other studies have reported delays in defibrillation that included prolonged pre and post shock pauses in chest compression (Edelson et al, 2006), inappropriate defibrillation (Kramer-Johansen et al, 2007) and hyper-ventilation (O’Neill & Deakin, 2007; Treanor & Spearpoint, 2007).
Whilst this evidence has informed our thinking about the performance of ‘work’ in resuscitation, my experience and that of colleagues, continues to suggest that we have yet to significantly understand & address many of the performance shortfalls identified – both from an educational perspective (in our resuscitation training courses), but more importantly, in the field whilst actively engaged in resuscitation.
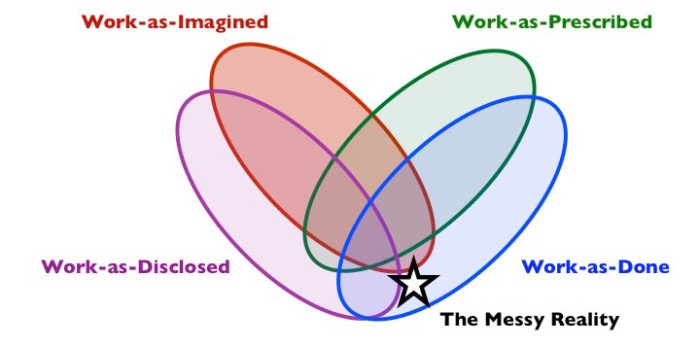
Moreover, there is evidence of miss-placed, but well-intentioned practices, that attempt to address some of the ‘human factors’ issues that arise in resuscitation practice, which I have previous alluded to in a blog, (https://resuspanopticon.wordpress.com/2015/02/28/the-3-point-pulse-check-cardiac-arrest-patient-safety-an-als-myth-or-best-practice/). One cannot help but think that such situations arise in a lack of application of human factors understanding, specifically the gap between ‘work-as-prescribed’ / ‘Work-as-Imagined’ and ‘Work-as-Done?
Human Factors Education in Life Support Courses
The development of team leadership skills has been stated as a key learning outcome in the UK ALS course, however, when one considers the current standards for in-hospital resuscitation teams (Resuscitation Council UK, 2010) it could be argued that leadership has never been appropriately assessed within the national Advanced Life Support course.
The Cardiac Arrest Simulation Test (CASTest) requires that the person being tested is able to lead a (small) team of ALS instructors through a low-fidelity, simulated cardiac arrest scenario. As many who read this will know, one of the instructors guides the student through the assessment and completes a checklist. Successful completion of the CASTest is achieved if the student is able to recall and provide resuscitation by following the correct and appropriate sequence of treatment in accordance with the decision algorithm (‘work-as-prescribed’).
Over the years, many have experienced difficulties during the CAStest, specifically where there remains considerable doubt as to a candidate’s genuine ability to co-ordinate and direct a real cardiac arrest, despite having satisfied all of the criteria on the assessment checklist – many instructors have been heard to say things like; “…the candidate ‘ticks all the boxes’, but I wouldn’t want them resuscitating a member of my family…”. The elements of our doubts being closely aligned to the characteristics identified in the work of Patterson and colleagues (2015) outlined above. Herein lies a paradox between ‘work-as-prescribed’ and ‘work-as-done’, what exactly are the issues that lead ALS instructors to question the validity of the assessment checklist and doubt the real-life abilities of the person being tested?
It is important to recognise that in recent years that the language of human factors / non-technical skills has appeared with increasing frequency of use within the didactic educational materials of the UK advanced life support course (ALS), which has seen an amended version of the TEAM tool (Cooper et al, 2009) incorporated into the CASTeach (cardiac arrest simulation teaching station). However this has not as yet transferred into the criteria within the ALS CASTest (cardiac arrest simulation test). Some would even argue that summative assessment may not be necessary at all (depending on one’s pedagogical position).
Perhaps we have reached a point where we need to narrow the gap between ‘work-as-prescribed’ and ‘work-as-done’ and place an increased focus on limiting performance variability through better teaching and facilitation of deliberate practice of complete task resuscitation with more time for deeper, broader debriefing. Another important adjustment might be in modifying the approach towards an educational experience (in a psychological safe space) that better prepares participant to systematically co-ordinate and direct an optimal resuscitation attempt?
The model of used in the Advance Resuscitation of the Newborn Infant (ARNI) course, which uses structured simulation teaching would appear to be more fit for purpose and instructors / medical educators have (informally) reported a high-level of satisfaction (https://www.resus.org.uk/information-on-courses/advanced-resuscitation-of-the-newborn-infant/).
Increasing our awareness of the complexity of work in clinical resuscitation through developing an understanding human factors/ergonomics may reap outcome benefits for patients. Being mindful of the significant challenges faced by clinicians in their clinical decision-making is yet to effectively penetrate our educational attention and little of the evidence thus far amassed has been applied the complexities of managing cardiac arrest.
To quote Martin Bromiley in the excellent video Just a Routine Operation (https://vimeo.com/970665 ) “we need to wake up to human factors”.
References
Abella, B., Edelson, D., Kim, S., et al. (2007). CPR quality improvement during in-hospital cardiac arrest using a real-time audiovisual feedback system. Resuscitation. 73. 54-61.
Acute Care – Quality Standards for CPR (2010). Resuscitation Council UK. https://www.resus.org.uk/quality-standards/acute-care-quality-standards-for-cpr/#team
Bion, J.F., Abrusci, T. and Hibert, P. (2010) Human factors in the management of the critically ill patient. British Journal of Anaesthesia. 105 (1). 26-33.
Bucknall, T. (2010) Medical error and decision making: Learning from the past and present in intensive care. Australian Critical Care. 23. 150-156.
Center for Evidence Based Medicine. http://www.cebm.net/index.aspx?o=1036 [on line]. Retrieved 05/12/2015.
Cooper S, Cant R, Porter J, Sellick K, Somers G, Kinsman L, Nestel D. (2010). Rating medical emergency teamwork performance: development of the Team Emergency Assessment Measure (TEAM). Resuscitation. 81(4):446-52.
Edelson, D.P., Abella, B., Kramer-Johansen, J., et al. (2006) Effects of compression depth and pre-shock pauses predict defibrillation failure during cardiac arrest. Resuscitation. 71. 137-145.
Guyatt, G.H. et al. (2008). GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 336. 924-926.
Gwinnutt, C., Columb, M. and Harris, R. (2000) Outcome after cardiac arrest in adults in UK hospitals: effect of the 1997 guidelines. Resuscitation. 47(2).125-135
Kramer-Johansen, J., Edelson, D., Abella, B., et al. (2007) Pauses in chest compression and inappropriate shocks: a comparison of manual and semi-automatic defibrillation attempts. Resuscitation. 73. 212-220.
Nolan, J.P., Soar, J., Smith, G.B., Gwinnutt, C., Parrott, F., Power, S., Harrison, D.A., Nixon, E., Rowan, K. (2014). Incidence and outcome of in-hospital cardiac arrest in the United Kingdom National Cardiac Arrest Audit. Resuscitation.85(8).987-992.
Nolan, J.P. et al. (2015). Part 1: Executive summary 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Resuscitation 95. E1-E31.
O’Neill, J.F., and Deakin, C.D. (2007) Do we hyperventilate cardiac arrest patients? Resuscitation. 73(1) 82-5
Patterson, D.P., Pfeiffer, A.J., Lave, J.R., Weaver, M.D., Abebe, K., Krackhardt, D., Arnold, R.M. and Yealy, D.M. (2015). How familiar are clinician teammates in the emergency department? Emergency Medicine Journal. 32:258–262.
Peberdy, M., Kaye, W., Ornato, J., Larkin, G., Nadkarni, V., Mancini, M., Berg, R., Nichol, G. and Lane-Trultt, T. (2003). Cardiopulmonary resuscitation of adults in the hospital: a report of 14720 cardiac arrests from the National Registry of Cardiopulmonary Resuscitation. Resuscitation. 58(3). 297-308.
Reason. J. (1990). Human Error. Cambridge University Press. Cambridge.
Resuscitation Council UK (2010). Quality standards for cardiopulmonary resuscitation practice and training. https://www.resus.org.uk/quality-standards/acute-care-quality-standards-for-cpr/ retrieved 28/11/2015.
Treanor, G. and Spearpoint, K. (2007). Ventilation practice during in-hospital cardiac arrest. Resuscitation. 77.S2.
Whitfield, R., Colquhoun, M., Chamberlain, D., Newcombe, R., Davies, C.S., and Boyle, R. (2005). The Department of Health National Defibrillator Programme: analysis of downloads from 250 deployments of public access defibrillators. Resuscitation. 64. 269-277.